Abnormal Placentation
Familiarity with the underlying pathophysiology of abnormal development of the placenta (abnormal placentation) and its known clinical associations is of paramount importance, as adverse perinatal outcomes are associated with abnormal placentation.
The causes in the majority of abnormal placentation cases are unknown. Abnormal placentation is believed to be related to genetic, epigenetic, immune-genetic, immune, and local uterine factors. Other risk factors include preeclampsia, diabetes, smoking, and illicit drugs.
The four most common patterns of abnormal placentation/placental injury are:
A. Vascular:
1. Maternal vascular malperfusion
2. Foetal vascular malperfusion
B. Inflammatory:
3. Acute chorioamnionitis
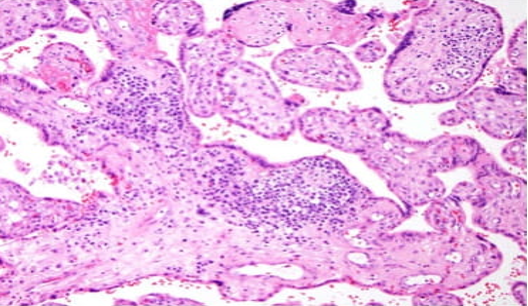
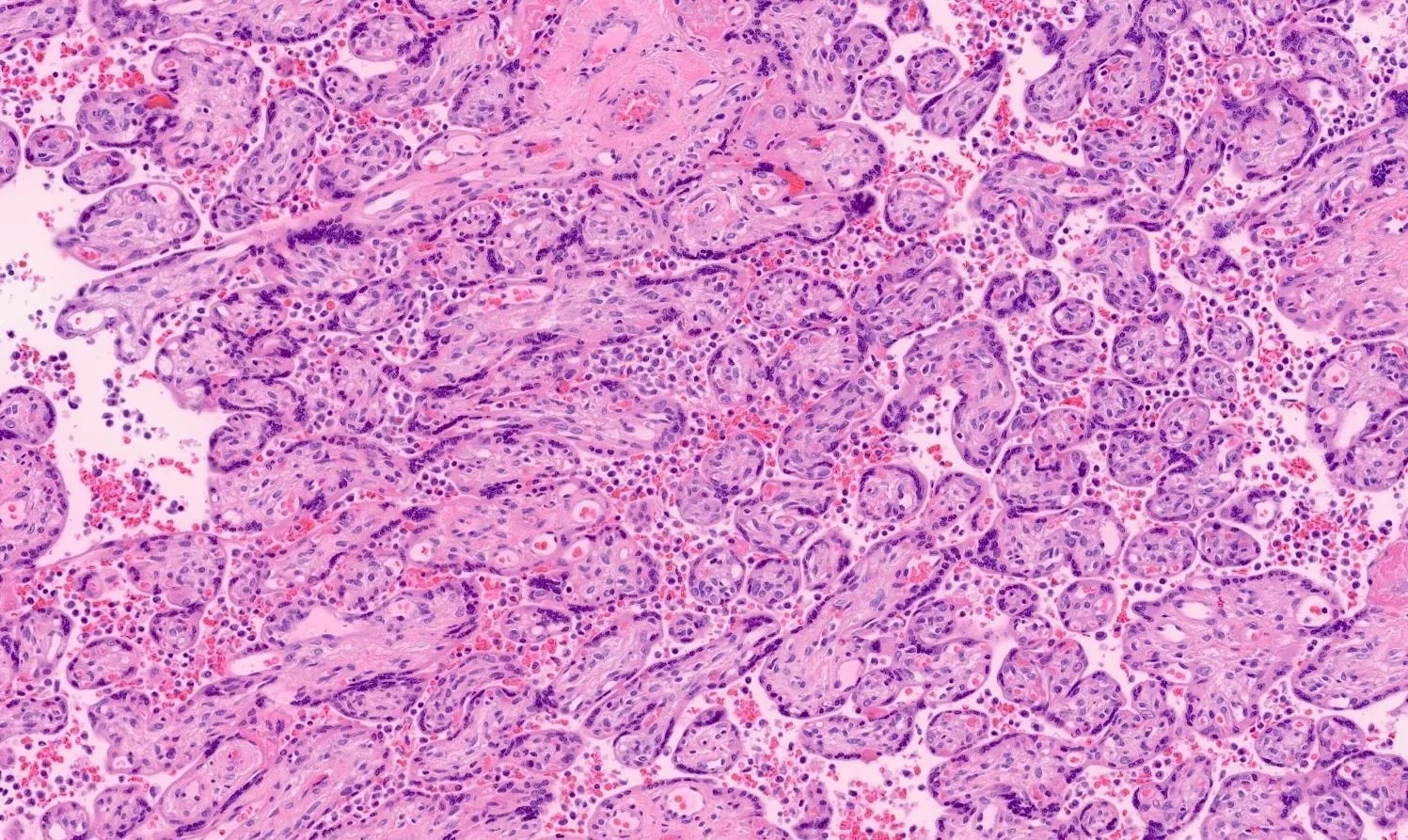
4. Chronic villitis of unknown etiology (non‑infectious)
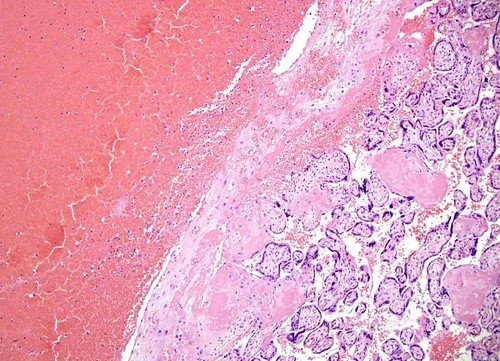
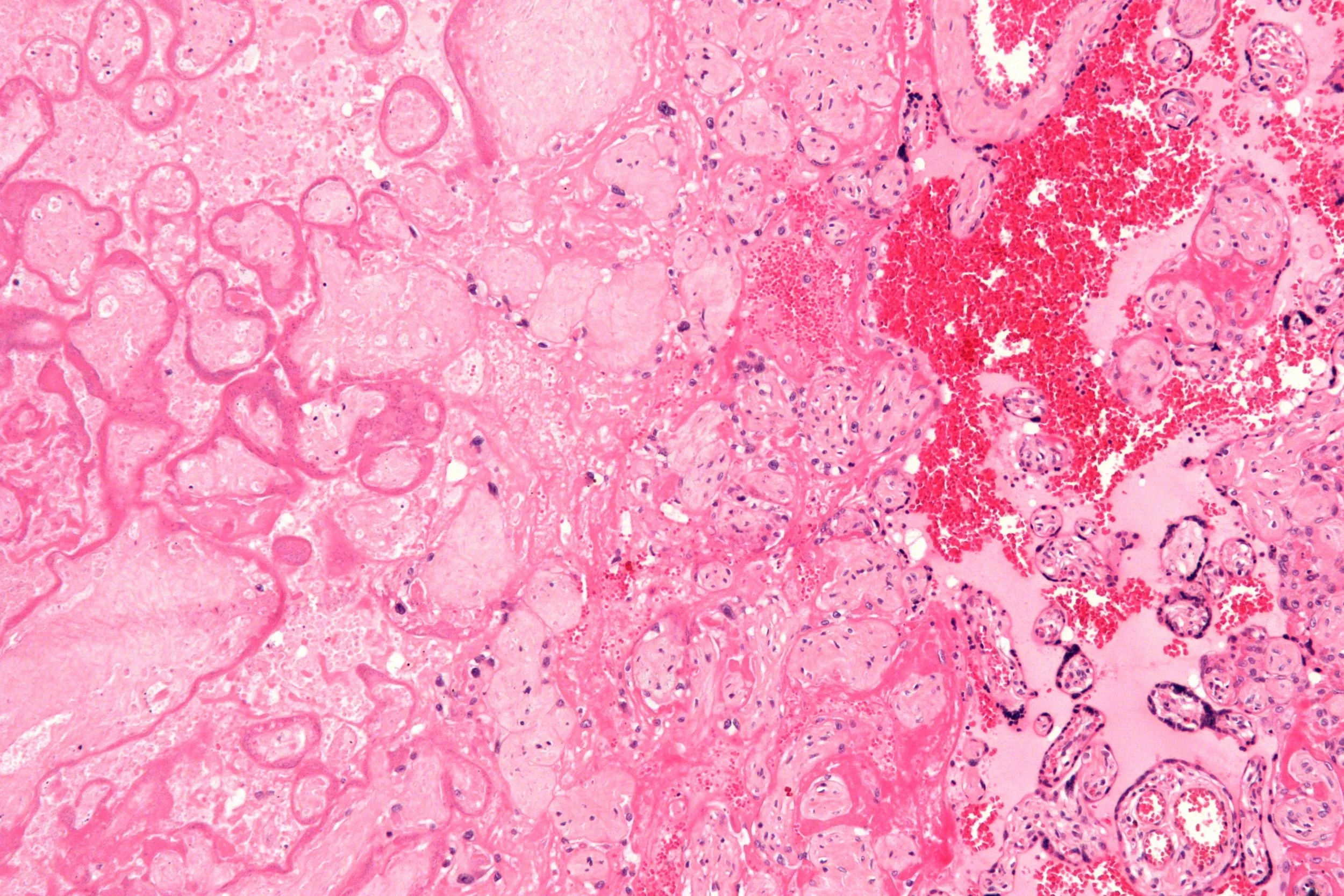
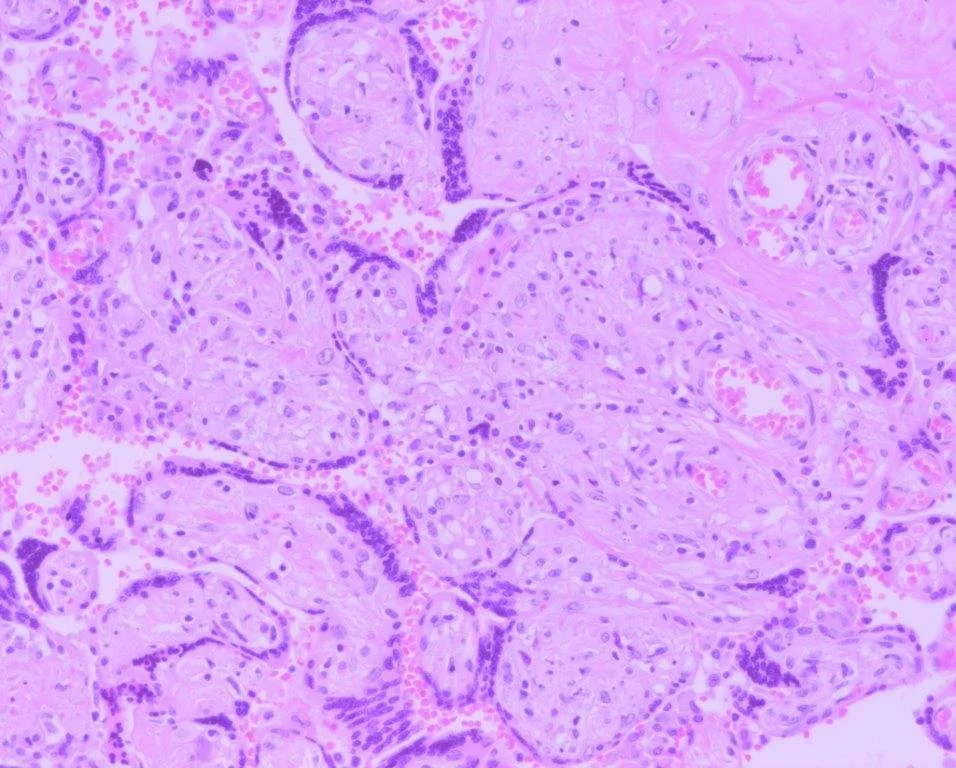
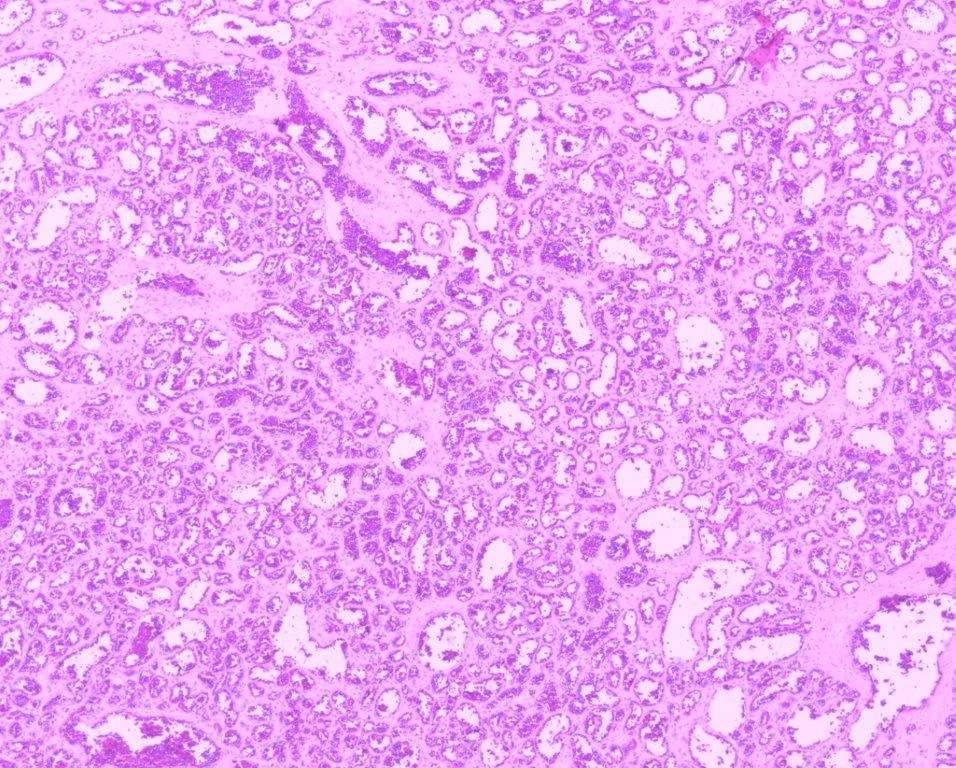
Other subtypes include massive perivillous fibrin deposition, placental infarcts, and chorioangiosis.
Healthy placentation and placental development throughout pregnancy are crucial to maintaining a healthy pregnancy, and so we monitor patients beyond their first trimester.
Our research and experience show a cohort of patients who experience repeated implementation failures or recurrent miscarriages are likely to be at higher risk in the second, or sometimes third, trimester.
For this cohort and others, immunotherapy is useful as a risk reduction strategy, as well as helping disease modification of abnormal placentation.
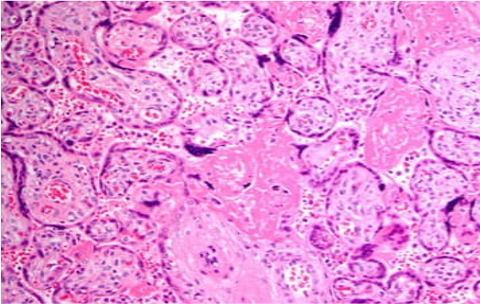
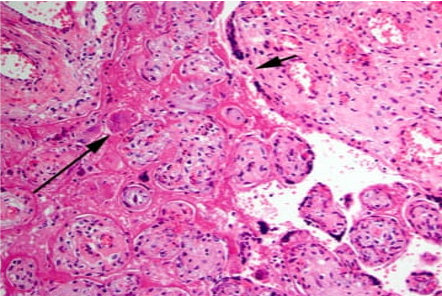
Examples of abnormal immune placentation